

Last month a patient walked into my office for a routine physical. He felt great. Exercised three times a week, slept well, no complaints. We ran the standard bloodwork and his lipid panel came back with LDL at 178, triglycerides at 340, and HDL at 36. Three numbers all going the wrong direction at once, and the man had no idea anything was off.
That’s what working with mixed hyperlipidemia looks like from my side of the desk. The condition rarely announces itself. People feel fine right up until the point where the damage that’s been building silently in their arteries finally causes a problem, and by then you’re dealing with something much harder to treat.
Quick Answer
Mixed hyperlipidemia is a lipid disorder where both LDL cholesterol and triglycerides are elevated at the same time, often with low HDL cholesterol. It affects roughly 1 in 100 people and is one of the most common genetic lipid disorders. The ICD-10 code is E78.2. It raises the risk of premature heart disease, stroke, and acute pancreatitis. Treatment involves statins for cholesterol, fibrates or omega-3s for triglycerides, and dietary changes focused on reducing saturated fats and refined carbohydrates.
What is mixed hyperlipidemia in medical terms?
It’s a metabolic disorder where multiple blood lipids are abnormal simultaneously. Mixed hyperlipidemia means your LDL cholesterol (the “bad” cholesterol) is too high, your triglycerides are too high, and often your HDL cholesterol (the “good” cholesterol) is too low. The medical name you’ll sometimes see on journal articles is familial combined hyperlipidemia, or FCHL.
If you’ve seen the code E78.2 on your medical chart or an insurance form, that’s what it refers to. Other related ICD-10 codes worth knowing: E78.0 for pure hypercholesterolemia (only LDL is elevated), E78.1 for pure hypertriglyceridemia, E78.5 for unspecified hyperlipidemia, and E78.49 for other types.
How it differs from regular high cholesterol
I explain this at least twice a week to patients, so I’ll put it simply.
Regular high cholesterol (pure hypercholesterolemia, E78.0) means your LDL is up but your triglycerides are fine. You take a statin, adjust your diet, and in most cases the problem is managed. Straightforward.
Mixed hyperlipidemia is a different animal because you’ve got two separate lipid problems happening at the same time. Statins lower LDL effectively but they don’t do much for triglycerides. So now you need a second medication on top of the statin, or you need to make specific dietary changes that target triglycerides separately. It’s a more complicated treatment plan, and that’s why the distinction between “high cholesterol” and “mixed hyperlipidemia” actually matters.
| Pure Hypercholesterolemia | Mixed Hyperlipidemia | Unspecified Hyperlipidemia | |
| ICD-10 | E78.0 | E78.2 | E78.5 |
| What’s elevated | LDL only | LDL AND triglycerides | Not clearly categorized |
| Triglycerides | Normal (<150 mg/dL) | Elevated (>150, often >200) | Variable |
| HDL | May be normal | Often low (<40 men, <50 women) | Variable |
| Treatment | Statins | Statins + fibrates/omega-3s | Depends on profile |
| Pancreatitis risk | Low | High if triglycerides >500 mg/dL | Variable |
Mixed hyperlipidemia symptoms
Here’s the part that makes my job harder than it should be: there usually aren’t any.
I’m serious. The overwhelming majority of patients I diagnose with this condition feel perfectly healthy on the day I tell them something is wrong. They came in for a routine check, or their employer required a physical, or their spouse nagged them into making an appointment they’d been putting off for two years. The lipid panel catches it. Their body didn’t.
That’s why the American Heart Association recommends starting lipid screening at age 20 and repeating it every 4 to 6 years. Conditions like this are invisible until they’re not.
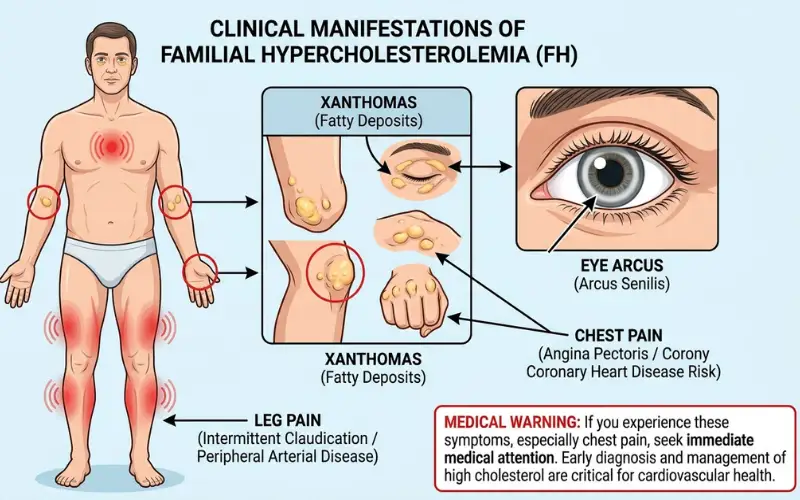
When physical signs do eventually show up, they typically mean things have been progressing for a while. Yellowish fatty deposits called xanthomas can appear on the skin, particularly around the elbows, knees, and along the Achilles tendon. There’s also a specific variant called xanthelasma that shows up as flat yellowish patches near the eyelids. I’ve learned to look for those during exams because spotting them early gives me a reason to order labs even if the patient has no complaints.
A whitish-gray ring around the iris called arcus cornealis is another sign. Common and harmless in older patients. In someone under 45, though, it catches my attention.
The symptoms of chest tightness, trouble breathing when exercising or pain in the calf muscle during walking are more likely to appear too late. If you’ve already developed plaque in your arteries, it probably isn’t going to get better if you take those supplements. At that stage we’re not preventing damage. We’re responding to it.
What causes mixed hyperlipidemia?
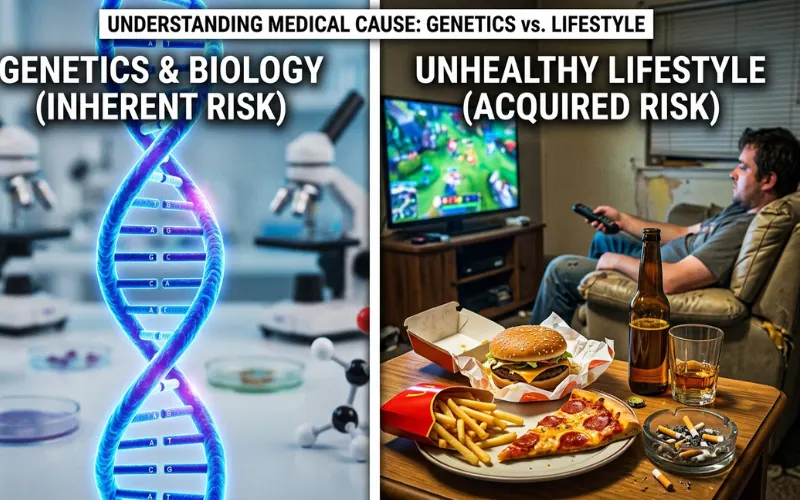
Genetics and lifestyle, working together. The inherited component makes you susceptible. The lifestyle factors determine how bad it actually gets.
FCHL runs in families. It’s polygenetic, which is why researchers believe that it’s several genes that play a role rather than one, and this is part of why even siblings in the same family can experience it differently. It is found in about 1 percent to 2 percent of people, based on National Library of Medicine statistics. If a parent has it, the odds of passing it on sit around 50 percent.
Something I’ve noticed over the years that often surprises people: FCHL can show up in the late teens. Early 20s. Most patients don’t associate cholesterol problems with that age group, but the genetic forms don’t wait until middle age.
Regarding lifestyle, the same old story goes. Having too much belly fat. Type 2 diabetes or even prediabetes (insulin resistance causes both LDL and triglycerides to rise). Undertreated thyroid problems. Drinking more than a couple times a week. A diet of white bread, fried food, pop and processed snack foods. Sitting for a prolonged amount of time. And some drugs (thiazide diuretics, certain beta-blockers and even corticosteroids) can lead at least one of the numbers into negative territory, even if patients are being as healthy as possible.
When the patient’s lipid numbers are elevated, my first question to the patient is, “Have you had any heart attacks before 55 in men and 65 in women? If it is yes, I’ll say no about their diet before I say FCHL.
How is mixed hyperlipidemia diagnosed?

Blood draw after a 9 to 12 hour fast. The fasting part matters because eating temporarily spikes triglycerides, which would throw off the reading and potentially mask or exaggerate the problem.
What I’m looking at on the results:
Total cholesterol above 240 mg/dL. LDL above 130, or above 100 if the patient already has other risk factors. Triglycerides above 150, with anything over 500 putting them in acute pancreatitis risk territory. HDL below 40 for men, below 50 for women.
No single number makes this diagnosis. It’s the combination that matters. High LDL alone is pure hypercholesterolemia. High triglycerides alone is pure hypertriglyceridemia. Both elevated together, often with low HDL, is mixed hyperlipidemia.
Why I’ve been ordering ApoB tests more often

Apolipoprotein B is a protein that is found on each LDL particle. Just measuring it will give you a better idea of how many LDL particles are in the blood, rather than measuring the total cholesterol that the LDL particles are carrying.
I’ve seen patients with a lower than normal LDL level, with elevated ApoB. This was because a lot of small dense LDL particles were in circulation. It is these smaller particles that penetrate into the wall of the arteries with the greatest ease. The standard LDL test missed the real risk. The ApoB test caught it.
The American College of Cardiology recommends ApoB testing for people with mixed hyperlipidemia, metabolic syndrome, or diabetes. It’s not something every doctor orders automatically yet, but it should be on your radar. If yours hasn’t mentioned it, bring it up.
How serious is mixed hyperlipidemia?
The honest answer: quite serious if nobody does anything about it.
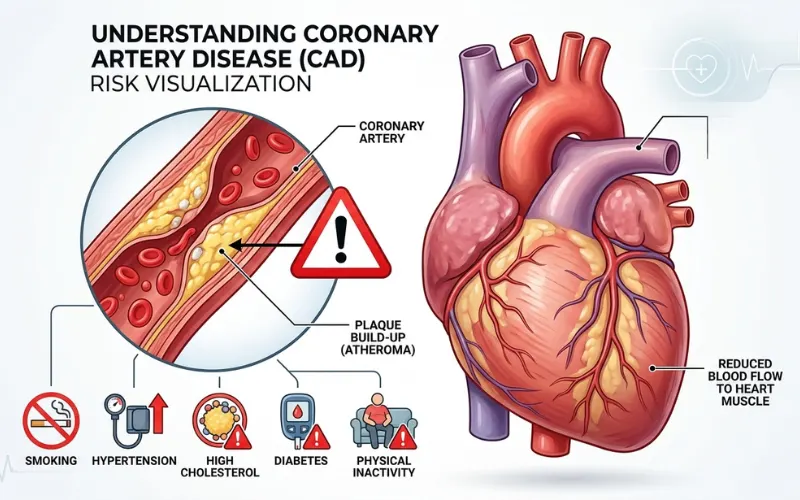
NIH data puts the risk of premature coronary artery disease at 2 to 5 times the baseline for people with untreated mixed hyperlipidemia. “Premature” means before 55 in men and before 65 in women. Those aren’t small increases.
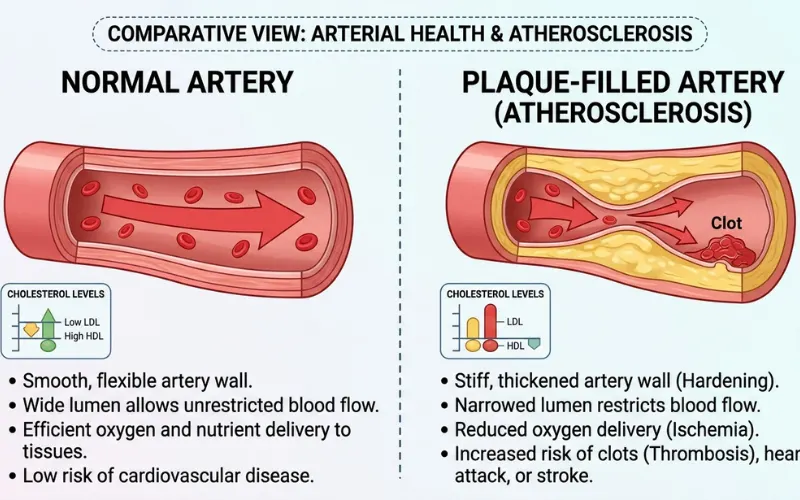
The reason the combined elevation is worse than either one alone comes down to how the damage accumulates. LDL deposits cholesterol into arterial walls. Chronically elevated triglycerides promote inflammation and the formation of small, dense LDL particles that are especially good at penetrating those walls. Low HDL means less cholesterol gets cleared back out. Everything compounds.
Separately from the heart, triglycerides above 500 mg/dL carry a real risk for acute pancreatitis. That’s an emergency, not a long-term concern. When I see triglycerides that high, bringing them down quickly becomes the immediate priority, sometimes even before addressing the LDL.
What about life expectancy?
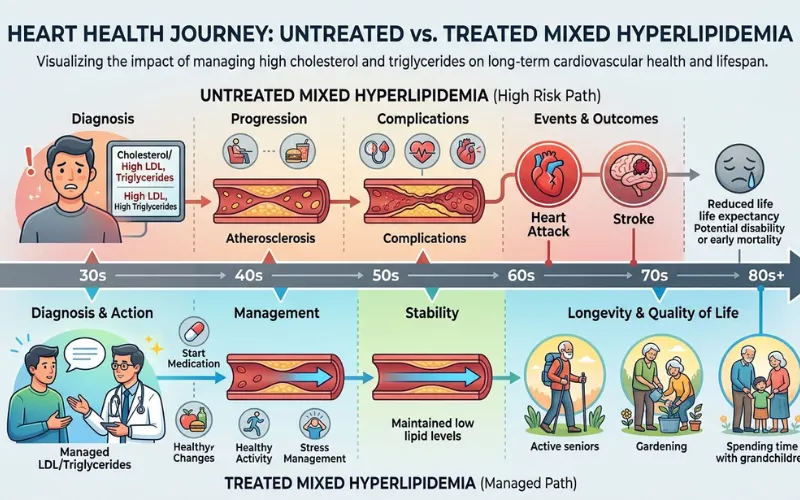
Studies in the Journal of Clinical Lipidology suggest untreated FCHL shortens life expectancy by 10 to 20 years. That reduction comes almost entirely from cardiovascular events: heart attacks and strokes hitting people who had decades of healthy years left.
Treated? Near-normal lifespan. That’s the part I want patients to actually hear. The diagnosis sounds scary. The prognosis with treatment is genuinely good. Statins, fibrates, dietary changes, and consistent monitoring bring the risk curve back down to something very manageable.
How do you get rid of mixed hyperlipidemia?
“Get rid of” is the wrong framing if the root cause is genetic. You can’t change your genes. But you can bring every single number on your lipid panel back into the normal range and keep it there indefinitely with the right approach.
Medications
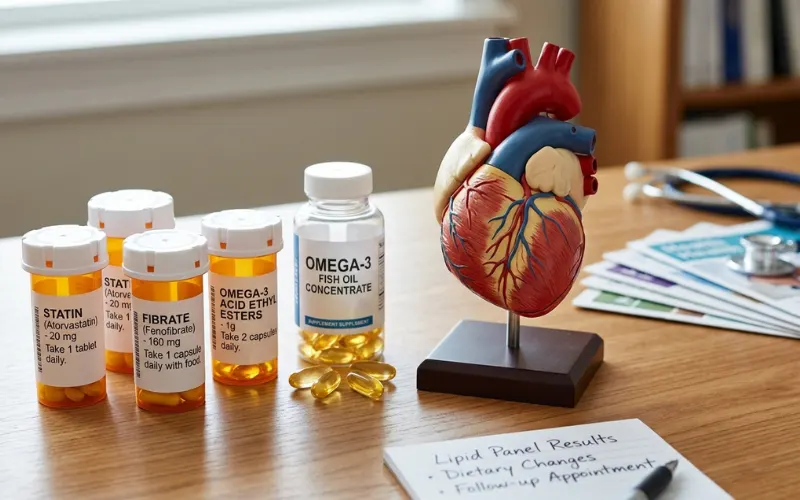
Nearly every patient I treat for this ends up on a statin. The top two drugs that I prescribe most are atorvastatin and rosuvastatin. They lower LDL 30 to 50 percent, depending on dosage, and has more clinical trials data than almost any class of drug used in cardiology.
There needs to be a solution for triglycerides. Fenofibrate is the most frequently used, as it can reduce triglycerides by 30-50% and can use it reasonably alongside a statin. But the two are not without problems. Usually a statin is used in combination with the fibrate, resulting in a higher risk of a muscle related side effect (myopathy), so I monitor CK levels occasionally, and instruct patients to let me know right away if they’re experiencing any unexplained muscle pain.
When prescription omegas 3 fatty acids, specifically Icosapent ethyl (brand name Vascepa), have been shown to be effective in reducing cardiovascular events, adding it on top of statins, they have gained a great deal of credibility from the REDUCE-IT trial. It’s a significant number. Made use of it for a couple of treatment regimens over the past year with patients who did not achieve adequate triglyceride level control with fibrates alone.
If the LDL persists despite taking statins to the maximum, I’ll add in ezetimibe, which prevents cholesterol stomach absorption, and will reduce the LDL by another 15 to 20 percent. For a small number of people who cannot tolerate cholesterol-lowering drugs or who do not get the desired results from taking cholesterol-lowering drugs, the final course of action is the PCSK9 inhibitor drugs such as evolocumab or alirocumab. Expensive and injected, but they lower LDL by 50–60 percent. I have used these quite a handful of times.
Can the numbers actually go back to normal?
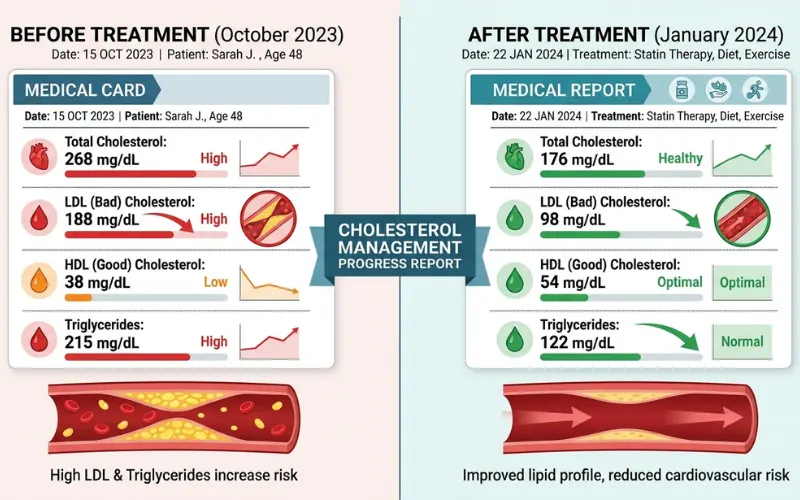
Yes. I see it regularly. A person walks into the office with the LDL being 180 and the triglyceride level is 400. Both are within normal range after six months of medication + actual diet adjustments.
The catch: stop the treatment and they climb right back up. The underlying tendency is permanent even when the numbers are controlled. This isn’t a temporary thing like a course of antibiotics. It’s ongoing.
What should I eat if I have mixed hyperlipidemia?
This is where I spend the most time with patients because the dietary advice for mixed hyperlipidemia doesn’t match what most people expect.
Everyone comes in thinking they need to cut fat. And reducing saturated fat does matter. But the thing that moves triglycerides the most in my experience isn’t fat reduction. It’s sugar and refined carb reduction. White bread. Pasta. Pastries. Soda. Sweetened coffee drinks. Fruit juice, which people think is healthy but is basically sugar water without the fiber.
I had a patient a couple years ago, triglycerides at 380, and we’d been going back and forth about medication. He asked if he could try diet first. Fine. I told him to keep the statin but swap every sugary drink for water, switch white bread for whole grain, and eat salmon twice a week. Came back in three months with triglycerides at 160. That case sticks with me because it showed how much targeted dietary changes can move the needle when the patient actually follows through.
What to eat more of
- Fatty fish twice a week. Salmon, mackerel, sardines. The omega-3 fatty acids bring triglycerides down directly.
- Soluble fiber from oats, barley, beans, lentils. It binds cholesterol in the gut and pulls it out of the body. The American Heart Association recommends 10 to 25 grams of soluble fiber daily.
- A handful of almonds or walnuts. Olive oil for cooking instead of butter. Vegetables in whatever amount you want, the more the better.
What to pull back on
- Refined carbohydrates are the priority for triglyceride control. Cut the soda. Cut the white bread. Reduce the pasta and pastries. I know nobody wants to hear that, but it works faster than most people expect.
- Saturated fat below 7 percent of daily calories. Less red meat, less full-fat dairy, less fried food. Zero trans fats from partially hydrogenated oils.
- Alcohol is a direct triglyceride raiser. Even two or three drinks a week can push numbers up in someone who’s already predisposed. If triglycerides are above 300, I tell patients to cut it out completely until we get the numbers down. Not a fun conversation, but an honest one.
What a realistic day looks like
Breakfast: oatmeal with walnuts and blueberries, no sugar. Lunch: chicken salad with olive oil dressing, cup of lentil soup. Dinner: salmon, roasted broccoli, quinoa. Snacks: apple with almond butter, carrots and hummus.
Normal food. Grocery store food. Nothing that requires a specialty shop or a nutrition degree to prepare.
When to see a doctor

If heart disease runs in your family, particularly heart attacks before age 55 in men or 65 in women, get a fasting lipid panel. Even if you’re 25 and feel invincible. The genetic forms of this condition don’t care how old you are.
If you’ve been diagnosed and you’re on medication, stay on it. I lose count of the patients who stop their statin because their numbers improved and they “feel fine now.” The numbers improved because of the statin. That’s how it works. Pull the medication and they come right back.
Chest pain, sudden shortness of breath, or severe abdominal pain (especially if your triglycerides have been high) are emergency-room situations. Don’t wait for a scheduled appointment.
Read Next: Medical Oversight for Wellness Clinics: Ensuring Safety
")